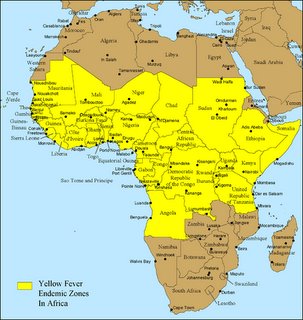
Map: Yellow Fever Belt, from CDC website
The first website that should be visited is the Travel section from the
CDC (Center for Disease Control). The
World Health Organization also has a good downloadable PDF outlining all the bugs that should keep you up at night worrying how to avoid. See their travelers health section, followed by the PDF titled “Vaccine-preventable diseases, vaccines and vaccination”
HIGHER PRIORITY
Although it seems as if there are an innumerable number of infectious agents that one has to be concerned about in a Tanzanian outdoor adventure, some things need to be considered higher priority based on chance of exposure, severity of illness, as well as what can be done to prevent/treat the infections. In my opinion, the main bugs we need to be concerned about are MALARIA AND GASTROINTESTINAL (foodborne, fecal-oral) illnesses that include: travelers diarrhea (EColi), cholera, Hepatitis A, and Typhoid Fever. In the U.S., there are no vaccines for travelers diarrhea or cholera (effective vaccines are available for cholera in certain countries), and not all cases of travelers diarrhea and cholera need antibiotic treatment, although this may be necessary in severe cases. Two vaccines that I think are essential include HEPATITIS A (2 shots, six months apart) and TYPHOID (the live oral form is good for 5 years, while the intramuscual injected version is good for two years). Another key vaccine includes TETANUS/DIPHTHERIA (Td), and should be administered every ten years.
There is no malaria vaccine, but malaria prophylaxis is effective in preventing infection if taken correctly. Malaria prophylaxis needs to be started at least a week before, for
mefloquine, or a day before travel in the case of
malarone(atovaquone/proguanil). Although doxycycline can also be used for malaria prophylaxis, it’s probably not a good choice since it can increase sun sensitivity… not a good thing standing exposed on top of Kilimanaro. Thus, the choice between mefloquine versus malarone is an individual decision. Mefloquine is cheaper, and is more convenient in that it is taken once weekly. However, neuro-psychological side effects are not uncommon, such as insomnia, bad dreams, and in worse cases, psychosis. The only documented mefloquine resistance is in the Thailand forests. Malarone has minimal side effects, but is more expensive (may be an issue since some insurance policies won’t cover this cost) and has to be taken daily.
LOWER PRIORITY
Again, lower priority doesn't mean less important, but overall chances are less (for our specific group) in encountering them. Booster shots for MEASLES and POLIO are recommended, but on a standard Tanzania safari and Kilimanjaro trek, it is unlikely that we will have exposure to these agents. The same goes for the MENINGIOCOCCAL vaccine (NEISSERIA MENINGITIDIS). Both polio and N. meningitidis can be found in western and central Africa, but in Tanzania, these bugs don’t appear to be a problem currently. HEPATITIS B vaccine is something to consider, but unless you are unfortunate to receive a contaminated blood transfusion, frequent some local bordello, or are into sharing needles for injectable recreational drugs, this is unlikely to be a problem.
For the YELLOW FEVER VACCINE, according to the CDC website as well as the WHO recommendations, this is not a REQUIREMENT when traveling directly from the U.S. to Tanzania, even though Tanzania is in the yellow fever belt. CDC does RECOMMEND the vaccine, however. Although there are a few exceptions, most countries located in the yellow fever belt require yellow fever vaccinations only if traveling FROM another country in the yellow fever zone TO their own country. In other words, they want to try to keep yellow fever from being imported into their country... they personally don't care if you catch it. However, the
U.S. State Department website adds some confusion to this, simply stating that a yellow fever vaccination is REQUIRED, not really specifying whether this means everybody, or only travelers coming from yellow fever regions. This is incorrect...we checked. Nonetheless, the need for YF vaccine will continue to be a source of confusio... its probably easier to just get it. The
CDC website also contains lists of clinics that are authorized to administer the Yellow Fever vaccine.
Since our safari is at the end, fortunately if we start developing undifferentiated fevers from AFRICAN TICKBITE DISEASE (Rickettsia africae) and/or AFRICAN SLEEPING SICKNESS (Trypansoma bruceii rhodesia) we will hopefully be back in the U.S. Both of these diseases are increasingly report from persons returning from safaris in Tanzania. There is no vaccine for either, and they can cause severe/fatal disease if not treated early. Avoiding ticks and tse-tse flies are the best one can do to avoid getting these bugs.
BOTTOM LINE
I ended up getting Yellow Fever vaccine, even though its not required coming from the U.S.…it’s good for 10 years and who knows I may need it in the future. We have also heard stories where people have been hassled for not having it, and in some cases made to be paid essentially a bribe to enter a country despite YF vaccine not being a requirement. Paying the $100 cost of the vaccine is probably worth avoiding the trouble by not having it. I got another typhoid vaccine (intramuscular) as well (my last one was > 3 years a go). I'm going with mefloquine for malaria prophylaxis. Although I’ve never taken this before, since I will be starting before we leave the U.S., if I end up with bad side effects, I’ll have time to switch to Malarone.
A list of meds we plan on bringing for prophylaxis, treatment, etc. It's overkill to some extent, but we have access to them, so why not. The number of tabs is based on four persons
--doxycycline (lepto, rickettsial, cholera) 100mg x 14 tabs
--levofloxacin 500mg x 14 tabs (typhoid, soft tissue, travelers diarrhea)
--pepto bismol (bismuth subsalicylate) 262mg tab 60 tabs
--ibuprofen 600 x 60
--compazine 5mg x30 tabs
--diamox (acetazolamide) 250mg three times day, 7 days x 4 persons = 84 tabs (for altitude illness)
--imodium
--DEET 10-30% Skin; clothes Permethrin
--claritin 10mg x 20
--flagyl
--dexamethasone 2mg tabs and nifedipine for treatment of HAPE and HACE, respectively
Labels: Drugs, Preparation, Vaccines















